Angiotensin converting enzyme (ACE) inhibitors and angiotensin receptor blockers in COVID-19
March 23, 2020
Jeffrey K Aronson, Robin E Ferner (University of Birmingham)
On behalf of the Oxford COVID-19 Evidence Service Team
Centre for Evidence-Based Medicine, Nuffield Department of Primary Care Health Sciences
University of Oxford
Correspondence to cebm@phc.ox.ac.uk
PDF to download
BMJ Editorial: Drugs and the renin-angiotensin system in covid-19
UPDATED 31st March 2020
It has been suggested that angiotensin converting enzyme inhibitors (ACE-1 inhibitors), such as enalapril and ramipril, and angiotensin receptor antagonists (colloquially called angiotensin receptor blockers or ARBs), such as candesartan and valsartan, may be of value in preventing and treating the effects of the coronavirus SARS-CoV-2 (also known as 2019-nCoV), the cause of the infection called COVID-19.
However, there is as yet no trial evidence of efficacy, and little attention has been paid to the possibility of harms from the use of such interventions or in what ways the balance of potential benefits and harms differ among individuals.
Currently (as of 21 March, 2020) three relevant trials are listed on the WHO’s website ICTRP, the International Clinical Trials Registry Platform, as having been proposed or being in progress in China. The first, titled “Clinical characteristics difference between the hypertension patients with and without ACEI treatment when suffered with 2019-nCoV infection in China” was registered on 12 February and is said to be recruiting; it is also listed on clinicaltrials.gov. The two others are not recruiting: “Recombinant human angiotensin-converting enzyme 2 (rhACE2) as a treatment for patients with COVID-19” (registered on 21 February but listed on clinicaltrials.gov as withdrawn) and “Clinical study for the effects of ACEIs/ARBs on the infection of novel coronavirus pneumonia (CoVID-19)” (registered on 2 March).
Here we review the pharmacology of these drugs and the mechanisms whereby the virus infects cells. Based on this analysis we make conclusions about whether these drugs should be used while we wait for the results of clinical trials.
The main questions to be asked are whether these drugs have any role to play in treating COVID-19 or conversely whether individuals currently taking these drugs should stop taking them in advance of an infection or at least when an infection occurs.
- The renin-angiotensin system and its inhibitors
A simplified version of the pharmacology of the renin–angiotensin system is shown in the diagram below.
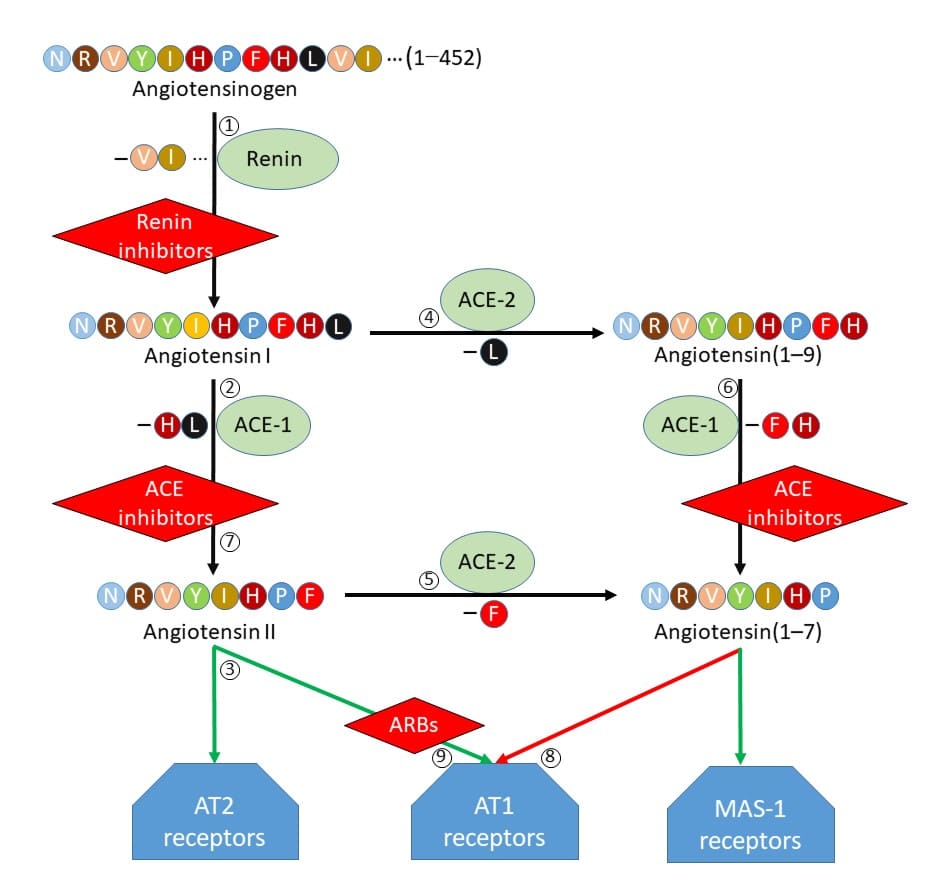
Figure 1. The renin-angiotensin system and its inhibitors and antagonists
Here are the main features of this scheme. The numbers in the list correspond to the numbers in the diagram::
- Angiotensinogen is converted to angiotensin I by renin.
- Angiotensin I (a decapeptide) is converted by ACE-1 to angiotensin II (an octapeptide).
- Angiotensin II is an agonist at both angiotensin AT1 and angiotensin AT2 receptors.
- Angiotensin I is also converted, by ACE-2, to the nonapeptide angiotensin(1-9).
- Angiotensin II is also converted, by ACE-2, to the heptapeptide angiotensin(1-7).
- Angiotensin (1-9) is converted, by ACE-1, to angiotensin(1-7).
- ACE-1 inhibitors inhibit the conversion of angiotensin I to angiotensin II and of angiotensin(1-9) to angiotensin(1-7). Inhibitors of ACE-2 have been developed, but none has been marketed.
- Angiotensin(1-7) is an antagonist at angiotensin AT1 receptors and an agonist at MAS-1 receptors.
- Angiotensin receptor antagonists block the actions of angiotensin II and angiotensin(1-7) at angiotensin AT1 receptors.
It is clear from this that the actions of ACE inhibitors and ARBs are complex, and the overall outcomes of using them in the context of COVID-19 are hard to predict.
- How SARS CoV-2 (2019-nCoV), the virus that causes COVID-19, infects cells (Figure 2)
Coronaviruses are single-stranded RNA viruses, about 120 nanometers in diameter. Their resemblance to the sun with a corona, as seen during an eclipse, is due to so-called spike glycoproteins, or peplomers, on the surface, which enable coronaviruses to enter host cells. SARS-CoV-1 and SARS-CoV-2, which share about 80% structural identity, do this by harnessing the action of the angiotensin converting enzyme, ACE-2, which is expressed in the membranes of many cells in the body, including lung alveolar epithelial cells.
The spike glycoproteins have two subunits; one subunit, S1, binds to the receptors on the cell surface; the other subunit, S2, fuses with the cell membrane. A host transmembrane serine protease, TMPRSS2, promotes entry of SARS-Cov into cells by two separate mechanisms. After the S1 subunit of the spike binds to the ACE-2 enzyme on the cell membrane surface, TMPRSS2 activates the spike and cleaves ACE-2. TMPRSS2 also acts on the S2 subunit of the spike glycoprotein, causing an irreversible conformational change, activating it, and facilitating fusion of the virus to the cell membrane. The virus then enters the cell. A model of these events is shown in Figure 2.
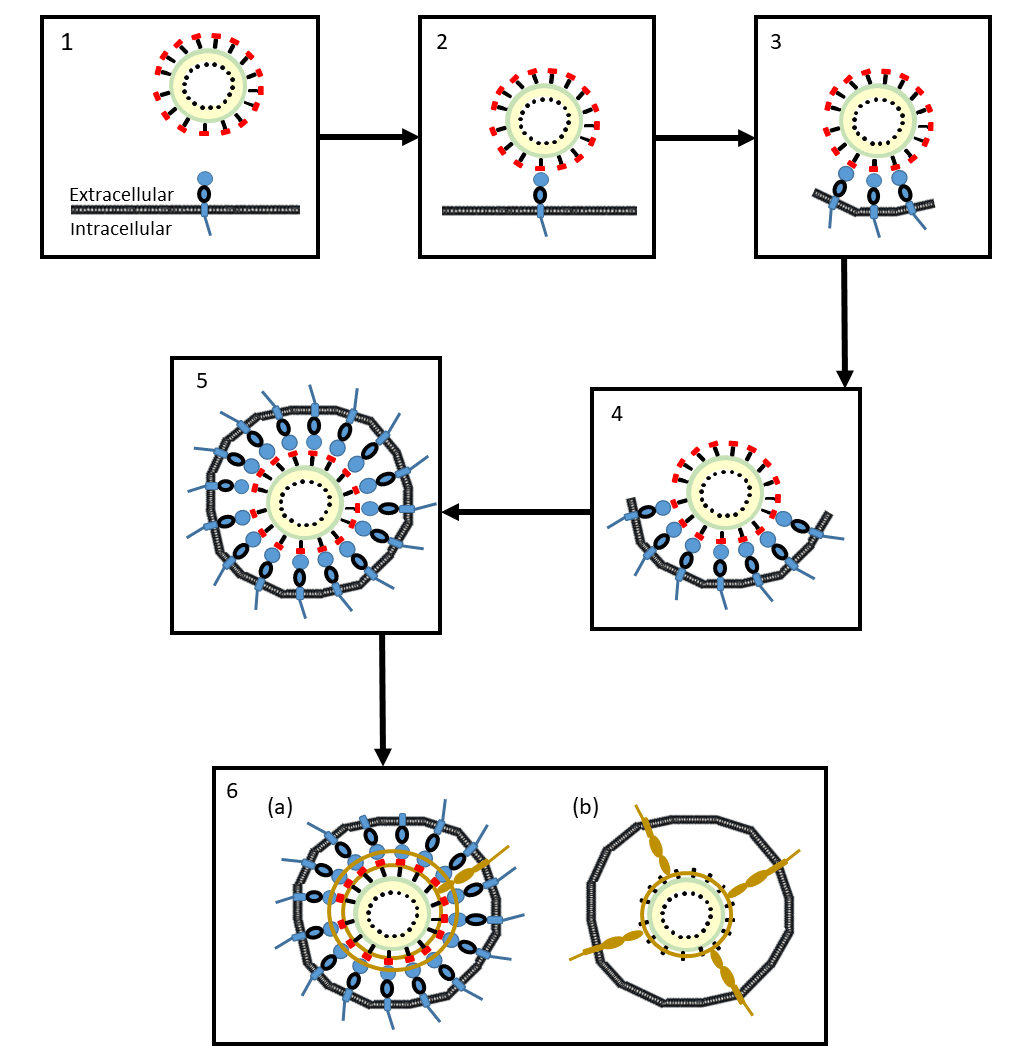
Figure 2. A proposed model of the mechanisms whereby coronavirus SRA-CoV-2 enters cells
- The coronavirus approaches the cell membrane
- An S1 subunit (red) at the distal end of a glycoprotein spike of the virus binds to a membrane-bound molecule of ACE-2 (blue)
- As more S1 subunits of the glycoprotein spikes bind to membrane-bound molecules of ACE-2, the membrane starts to form an envelope around the virus (an endosome)
- The process continues …
- … until the endosome is complete
- The virus can enter the cell in two ways:
(a) A cell membrane-bound serine protease (brown), TMPRSS2, cleaves the virus’s S1 subunits (red) from its S2 subunits (black) and also cleaves the ACE-2 enzymes; the endosome enters the cell (endocytosis), where the virus is released by acidification or the action of another protease, cathepsin
(b) The same serine protease, TMPRSS2, causes irreversible conformational changes in the virus’s S2 subunits, activating them, after which the virus fuses to the cell membrane and can be internalized by the cell
A serine protease inhibitor, camostat mesylate, used in Japan to treat chronic pancreatitis, inhibits the TMPRSS2 and partially blocks the entry of SARS-CoV-2 into bronchial epithelial cells in vitro.
- Analysis
Reducing the activity of ACE-2 in cell membranes could theoretically reduce the ability of SARS-CoV-2 to penetrate cells. However, ACE-1 inhibitors, such as enalapril and ramipril, currently used to treat hypertension and heart failure, do not inhibit ACE-2.
Inhibition of ACE-1 increases the concentration of circulating angiotensin I, which could be converted to angiotensin(1-9). However, the metabolism of angiotensin(1-9) to angiotensin (1-7) is catalysed by ACE-1 and would not proceed to any great extent in the presence of an ACE-1 inhibitor.
The presence of an increased amount of angiotensin I, due to inhibition of ACE-1, might tend to upregulate ACE-2. Indeed, in experimental animals ACE-1 inhibitors and ARBs both increase the activity of cardiac ACE-2.
It is not clear whether such upregulation would be desirable or not. Increased production of angiotensin(1-7) from angiotensin II under the action of ACE-2, despite reduced production from angiotensin(1-9) could lead to increased anti-inflammatory activity, partly mediated by inhibition of COX-2 synthesis, and some protection from the lung damage caused by the virus. However, since angiotensin II concentrations are reduced by ACE-1 inhibitors, that would be unlikely to be a large effect. In any case, increased anti-inflammatory activity by, for example, the administration of an NSAID or corticosteroids, may not be beneficial and could be harmful in virus infections. We note in passing that ACE-2 is upregulated by ibuprofen in experimental animals.
- Conclusions
- We do not know whether the supposed benefits of ACE-1 inhibitors or ARBs during an episode of infection with SARS-CoV-2 outweigh the potential harms.
- It is generally unwise to institute any pharmacological therapy on the basis of an untested mechanistic hypothesis, since unexpected harms may outweigh hoped-for benefits. Until evidence emerges, based on randomized trials or at least data-mining of patients’ records, we suggest that it would be unwise to use either conventional ACE-1 inhibitors or ARBs to treat COVID-19.
- Patients who are already taking ACE-1 inhibitors or ARBs have generally been advised to continue taking their medicines. The Council on Hypertension of the European Society of Cardiology has highlighted the lack of any evidence to support a harmful effect of ACE-1 inhibitors and ARBs in the context of the pandemic COVID-19 outbreak; however, lack of evidence does not demonstrate that the supposed benefit will outweigh the potential harms in infected patients. The American College of Cardiology has stated that “In the event patients with cardiovascular disease are diagnosed with COVID-19, individualized treatment decisions should be made according to each patient’s hemodynamic status and clinical presentation.” This is sensible advice.
- The most difficult decisions need to be taken in patients with severe hypertension or chronic heart failure, who may deteriorate rapidly if drugs acting on the renin–angiotensin system are withdrawn. There are two problems − treatment in advance of an infection and treatment during an infection:
– Continuing treatment in advance of an infection Those in whom these medications are most likely to be beneficial (i.e. those with severe hypertension or heart failure) are those in whom continued therapy is likely to be needed, and also those in whom adverse effects of COVID-19 are more likely and in whom it appears that mortality is increased in COVID-19. In the absence of more information, such patients should probably continue to take their medications.
– Continuing treatment during an infection In the absence of clinical trials in COVID-19, it is probably best to accept the proven benefits of continuing therapy for severe cardiovascular disease, and to continue therapy with ACE inhibitors or ARBs if an acute infection occurs, even at the uncertain risk of harms.
- Many patients with mild diabetes or cardiovascular disease or both will be taking these medicines for their long-term benefits; withdrawing treatment during an acute infection will cause little harm and is reasonable.
- Those who are deriving marginal benefit from these medicines, but who are at a high risk of infection because of exposure (e.g. younger healthcare workers) may reasonably stop taking these medicines during the epidemic; the adverse effects of drug withdrawal will be small and the risks of continuing therapy before and especially during an infection, albeit not quantified, may be greater.
- On recovery from the infection, treatment should be continued or resumed, as appropriate.
- This advice, summarized in Figure 3, is based on the theoretical considerations outlined above; it should be reviewed when the results of data mining patient records or clinical trials become available.
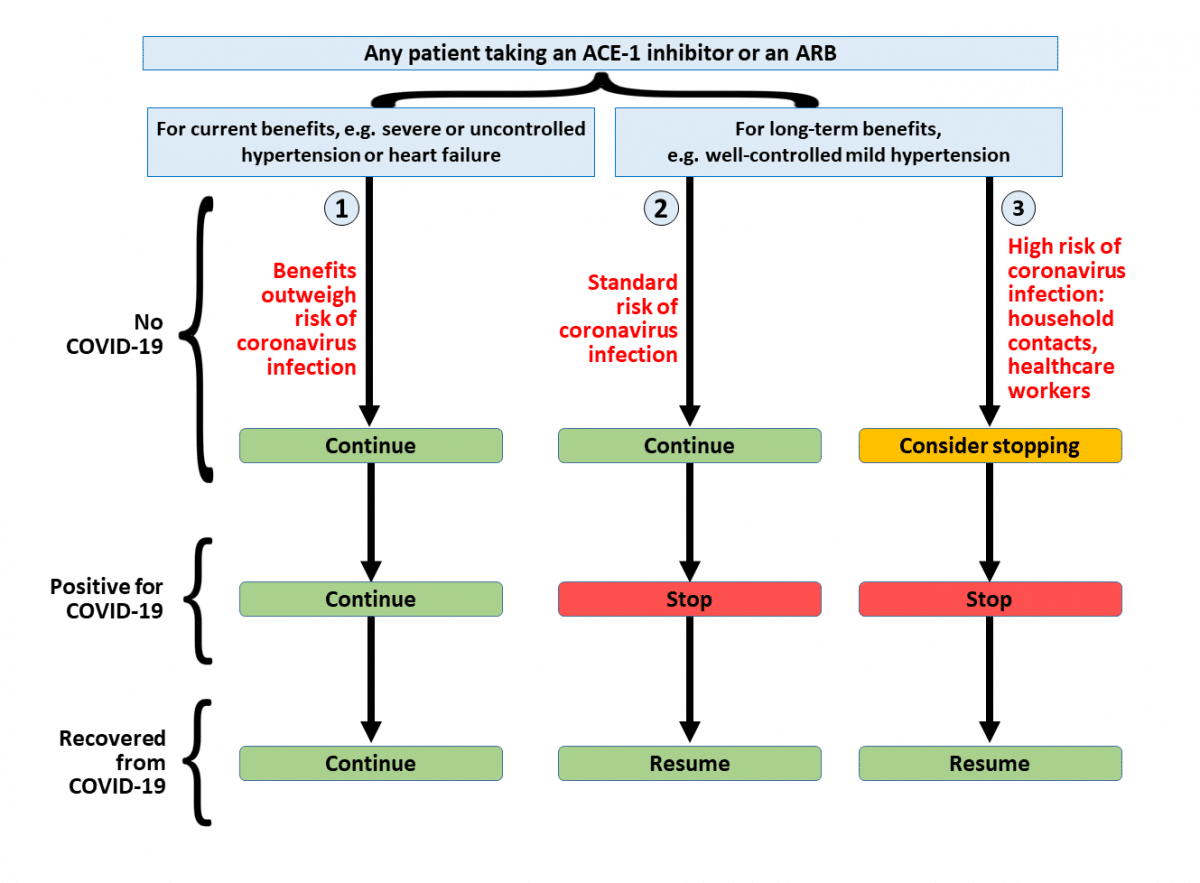
Figure 3. Advice on the continued use of ACE inhibitors and angiotensin receptor antagonists (ARBs) in individuals at risk of COVID-19 or who develop it:
Column 1: some, in whom the risks of stopping treatment are high, should continue to take their ACE inhibitors or ARBs, even if infection supervenes;
Column 2: advice to continue treatment will be suitable for most patients, unless they develop COVID-19;
Column 3: some patients in whom the benefits of ACE inhibitors or ARBs are small in the short term, and who have a high risk of COVID-19, may choose to stop taking their drugs until the epidemic is over
Acknowledgements
We are very grateful to Professor David Henry, Bond University, Faculty of Health Sciences and Medicine, Australia, and to others for reviewing our draft manuscript
Disclaimer: The article has not been peer-reviewed; it should not replace individual clinical judgement and the sources cited should be checked. The views expressed in this commentary represent the views of the authors and not necessarily those of the host institution, the NHS, the NIHR, or the Department of Health and Social Care. The views are not a substitute for professional medical advice.